Menopause Management: A Modern Clinical Roadmap
Written By: Dr. Janhvi Ajmera

Menopause is a universal milestone, but for many women, it doesn’t come quietly. Hot flashes, night sweats, disrupted sleep, and mood swings can turn daily life into a challenge and sometimes for years. For physicians, the task is clear but meticulous: how do we ease symptoms without exposing patients to unnecessary risks?
A recent JAMA review reframes this conversation by offering a structured, evidence-backed approach. But clinical guidelines are only as powerful as the way we apply them. Let’s unpack what this means for real-world practice and research.
Symptom Burden: More Than Just Hot Flashes
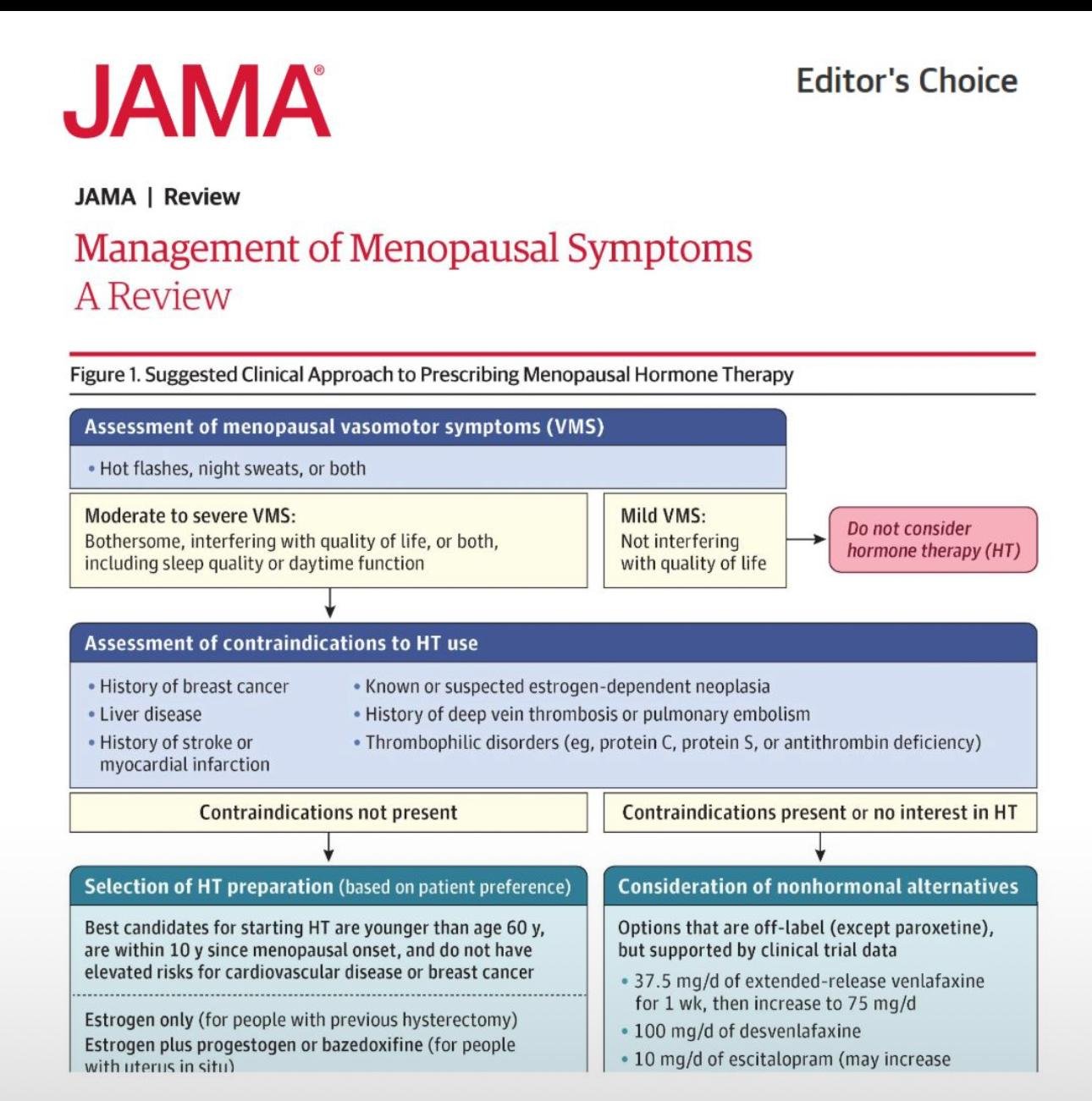
Nearly 8 in 10 women report vasomotor symptoms (VMS). For many, it’s more than discomfort; sleep disruption fuels fatigue, mood instability, and cardiovascular risk factors.
The clinical fork in the road is straightforward:
- Mild symptoms → tolerable, no significant impact → reassure and avoid overtreatment.
- Moderate to severe symptoms → interfering with daily life → treatment is justified, often transformative.
It sounds simple, yet underdiagnosis and undertreatment are global challenges.
The Safety Lens: First, Do No Harm
Hormone therapy (HT) is not for everyone. Before prescribing, clinicians must screen for red flags:
- History of breast cancer or estrogen-sensitive tumors
- Liver disease or impaired liver function
- Previous stroke, myocardial infarction, or thromboembolic disease
When contraindications are present, HT is off the table. When they’re absent, the door to therapy opens, but still with careful weighing of risks and benefits.
Hormone Therapy: The Right Patient, The Right Window
For the right candidate, HT can be life-changing. Best outcomes are seen in:
- Women under 60 years old
- Within 10 years of menopause onset
- Without elevated risk for breast cancer or cardiovascular disease
Treatment choices include:
- Estrogen-only therapy (for women with hysterectomy)
- Estrogen plus progestogen or bazedoxifene (for women with an intact uterus)
The guiding principle? Lowest effective dose, regularly reassessed. Route of administration (oral vs transdermal) should be personalized.
Beyond Hormones: The Nonhormonal Toolkit
Not all patients can or want to use HT. Fortunately, the nonhormonal armamentarium is growing, and clinical trial data are reassuring.
Evidence-backed alternatives include:
- SNRIs/SSRIs (e.g., venlafaxine, desvenlafaxine, escitalopram)
- Lifestyle strategies: structured exercise, weight management, cooling techniques, mindfulness-based interventions
For some, these are not just substitutes, they’re first-line solutions that respect safety and patient choice.
Clinical Pearls for Physicians
- Individualize always — menopause is a shared physiology but a unique experience for every patient.
- Don’t under-treat — severe VMS can erode quality of life and exacerbate comorbidities if left unmanaged.
- Think long-term — revisit treatment regularly; menopause care is a continuum, not a one-time prescription.
Research Horizons: Where Science Must Go
For biomedical researchers, menopause care represents an under-explored frontier. Key unanswered questions include:
- The molecular mechanisms behind hot flashes and thermoregulation
- Precision biomarkers to predict who benefits most from HT
- Safer nonhormonal agents with fewer side effects
- Longitudinal outcomes of early vs delayed HT initiation
This is where the next decade of translational science can directly transform millions of lives.
Final Word
Menopause isn’t a pathology, but poorly managed symptoms can feel like one. With evidence-based use of hormone therapy, nonhormonal alternatives, and personalized care, physicians can empower women to navigate this transition with strength rather than struggle.
Science and compassion must walk hand in hand. Menopause care isn’t only about reducing symptoms; it’s also about restoring quality of life.
REFERENCE:
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2833235?resultClick=1
Dual Antiplatelet Therapy: One-Size Doesn’t Fit All After PCI
Pregabalin & Heart Failure Risk: What Every Clinician Should Keep in Mind