
The IVIO Trial: Comparing Intravenous and Intraosseous Vascular Access in Out-of-Hospital Cardiac Arrest
Understanding Out-of-Hospital Cardiac Arrest
Out-of-hospital cardiac arrest (OHCA) is a frequent and life-threatening emergency with a high mortality rate. According to international guidelines, patients experiencing cardiac arrest with a nonshockable rhythm (asystole or pulseless electrical activity) should receive epinephrine, while those with a refractory shockable rhythm (refractory ventricular fibrillation or pulseless ventricular tachycardia) should receive epinephrine in combination with amiodarone or lidocaine.
To administer these life-saving medications during advanced life support, vascular access must be established. Both intravenous (IV) access and intraosseous (IO) access are commonly used for this purpose. While international guidelines recommend using IV access first, there is limited data supporting this recommendation.
The IVIO Trial: Comparing IV and IO Access
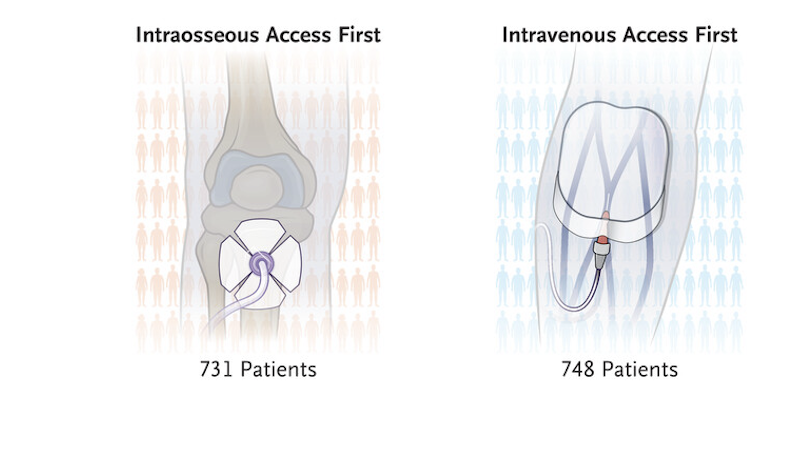
The Intravenous vs. Intraosseous Vascular Access during Out-of-Hospital Cardiac Arrest (IVIO) trial examined the effectiveness of IV versus IO vascular access in patients experiencing OHCA.
Key Findings
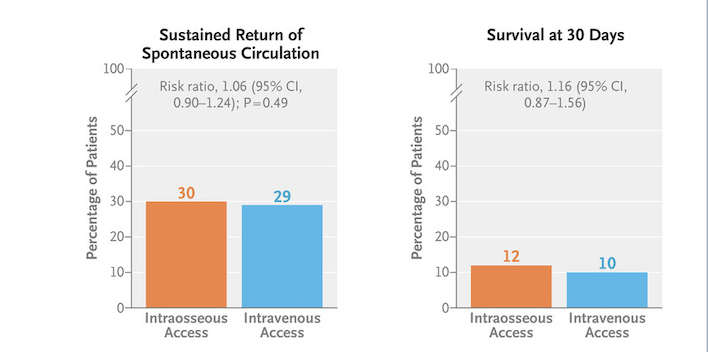
- The trial found no significant difference in sustained return of spontaneous circulation between patients who received intraosseous (bone) access and those who received intravenous (vein) access during out-of-hospital cardiac arrest.
- Despite current guidelines recommending IV access first, the use of IO access is increasing due to its perceived ease and speed, especially when IV access is difficult to establish during cardiac arrest.
- The study found that the time to first successful access and the time to first epinephrine administration were similar in both IV and IO access groups. This suggests that the route of administration does not significantly impact drug effects during cardiac arrest.
What Does This Mean for Emergency Care?
These findings challenge the traditional preference for IV access and highlight that both IV and IO access are viable options during cardiac arrest. Given that IO access is often faster and easier to establish in emergency situations, it may serve as a practical alternative when IV access is challenging.
Further research may be needed to evaluate long-term patient outcomes, but the IVIO trial provides important evidence that could shape future guidelines for vascular access in out-of-hospital cardiac arrest.
Follow @mdresearch.us on Instagram & visit mdresearch.us for more insightful content and blogs!